This article is an excerpt from We Organize to Change Everything: Fighting for Abortion Access and Reproductive Justice, a forthcoming ebook from Verso Books and Lux Magazine, available on June 15.
Abortion and transgender healthcare are provided at the intersection of shared oppressions: misogyny, and gender-based discrimination and violence. Over the last fifty years, the conservative right in the United States has created a playbook of anti-abortion legislation that is now being used to restrict access to trans health care. It is the responsibility of the reproductive justice and trans liberation movements to collaborate in our organizing strategies to defend life-saving health care—and further expand access.
The simultaneous criminalization of abortion in over half the United States while state after state attempts healthcare bans for trans youth is not a coincidence. It is critical for our movements to enter into this political moment with a fundamental historical understanding of the wins and losses that got us here. With access to care for both abortion and trans health care facing an onslaught of criminalization from right-wing political forces, a political understanding of shared roots in gender and gender-based oppression can help our movements build common struggle and solidarity, independent of a Democratic Party that has done next to nothing for us.
The Criminalization of Abortion
Roe v. Wade, the 1973 Supreme Court decision, declared it unconstitutional for the state to interfere with a pregnant person’s decision to access abortion prior to fetal viability (independent survival outside of the womb). Roe enshrines not a constitutional right to abortion but to privacy. In the movement it is said that “Roe is the floor, not the ceiling,” because it is the barest minimum of legal right to abortion in the US. We should have much more than Roe protecting abortion rights in this country. Abortion rights should not be imperiled by the death of an eighty-seven-year-old woman.
In 1994 another Supreme Court decision, Planned Parenthood v. Casey, reaffirmed the essential tenets of Roe, yet also provided new standards for what constituted permissible state restrictions on abortion rights. The primary change brought on by Casey was the qualifier on right to abortion without “undue burden” from the state. What constitutes an “undue” burden thus became a debate many state legislators were eager to have.
According to the preeminent research base for US reproductive rights, the Guttmacher Institute, 1,338 abortion restrictions have been enacted since Roe was decided, 108 in 2021 alone. Just in the first four months of 2022, 546 restrictions have been introduced in forty-two states while thirty-seven restrictions have been enacted in ten: Arizona (2), Florida (1), Idaho (1), Indiana (2), Kansas (1), Kentucky (18), Oklahoma (3), South Dakota (7), West Virginia (1), and Wyoming (1). These state-level restrictions have functionally ended abortion access for many and seek to undermine the legality of all abortion in the United States.
Abortion rights should not be imperiled by the death of an eighty-seven-year-old woman.
Mississippi is one of six states with only one remaining abortion clinic. Mississippi’s Gestational Age Act bans the termination of pregnancies after fifteen weeks. Legal challenge to this law reached the Supreme Court and the final decision on Dobbs v. Jackson Women’s Health will be handed down in a matter of weeks. The significance of Mississippi’s abortion ban lies not only in the hostile political battleground patients face if they attempt to access abortion in the South, but in the likelihood that the Supreme Court will uphold the law, transforming the legal basis of bodily autonomy nationwide.
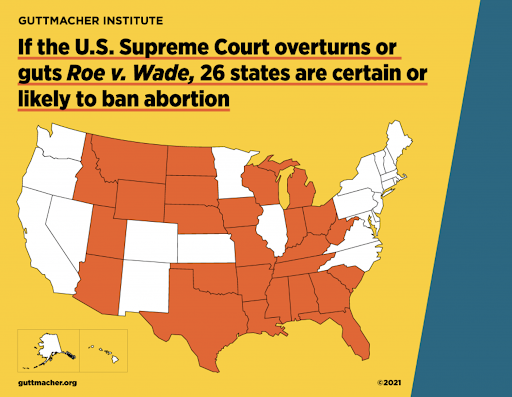
The May 2 leak of the Supreme Court majority opinion draft on Dobbs has confirmed what the abortion community has dreaded since the election of President Donald Trump: this decision will overturn Roe v. Wade. In the absence of Roe, abortion is likely to be criminalized in twenty-six states—either because those states do not have laws explicitly protecting abortion rights and will revert to pre-Roe legislation; or, the political environment of those states is such that severe abortion bans are all but inevitable. Near-total bans have already been passed at the state level over the last few months, kick-started by Senate Bill 8 in Texas.
Texas Senate Bill 8 (SB8) is a six-week abortion ban, passed in March 2021 and implemented six months later. It was at that time the most restrictive abortion ban to be enacted since abortion was legalized in 1973. SB8 also put forth new ways of criminalizing patients and providers, as it emboldened civilians to “see something, say something” if they suspected an abortion had been performed, encouraging abortion vigilantism by neighbors, family members, and care providers. This calls to mind Arizona’s racist anti-immigrant law, HB1070 (2010), which gave citizens license to call the cops on whomever they wanted if that person “looked like” someone undocumented. The Right clearly takes inspiration from every type of bigoted precedent they can find.
Many states are trying to pass copycat bills of SB8, as well as other bills with different severe restrictions. For example, Missouri’s HB2810 recently passed through the House and is awaiting hearing in the Senate. HB2810 would make the possession of abortion medications and equipment a felony in the state of Missouri. The original language of the bill included the treatment of ectopic pregnancy—non-viable pregnancies which are life-threatening medical emergencies. After harsh media and political criticism, mention of “ectopic pregnancy” was removed from the bill, but legislators reinforced that dispensing abortion medications to end an ectopic pregnancy would still be considered a felony under the law. The most absurd aspect of this extremism is the abortion medications, mifepristone and misoprostol, are not used to treat ectopic pregnancy. But anti-abortion politicians can’t resist kicking up a fuss, especially over something medically inaccurate.
Florida and Kentucky both passed fifteen-week abortion bans, similar to the Mississippi law currently before the Supreme Court. Kentucky’s legislature overrode a veto from the governor to pass HB3, which also created very stringent parental notification laws for people seeking abortions before they turn eighteen, including a signed and notarized parental consent from both parents.
The most severe ban passed this spring was a six-week ban in Oklahoma. Governor Kevin Stitt openly declared, “We want to outlaw abortion in the state of Oklahoma,” as he signed the bill into law which allows abortion only in cases where the pregnant person’s life is at risk (and not in the case of rape or incest, which are the other two common exceptions even for anti-abortion politicians). Otherwise performing abortions in the state of Oklahoma now carries a felony charge punishable by up to ten years in prison and a $100,000 fine. Kentucky and Idaho’s attempted bans were struck down almost immediately in court, while Tennessee’s law patterned after Texas’ SB8 has passed the House’s health subcommittee and awaits its next hearing.
When Roe is overturned, Illinois specifically is facing a catastrophe of unspeakable magnitude. Already Illinois is considered an oasis state for abortion access in the Midwestern US. Abortion bans and restrictions in surrounding states are so severe that their residents find it necessary to cross state borders to access abortion in Illinois. Assuming the Dobbs decision negates federal protection of pre-viability abortions, the number of people at risk for pregnancy whose nearest abortion provider is in the state of Illinois will go from 100,000 currently to almost nine million–an 8,651 percent increase.
The specific states where most people would come from are mostly Illinois border states, but also include other states like Ohio, Louisiana, Arkansas, and Mississippi—states hundreds of miles away. This illustrates how severe and far-reaching the repercussions of these bans are, and this is just Illinois data. This predicted exponential increase of the need for care in Illinois is very concerning to providers here. We are scrambling to put infrastructure in place to help accommodate such a massive influx of patients, but it is clear this is an impossible task.
One must also wonder what new layers of police and military presence at internal domestic borders may develop as different states seek to criminalize neighboring practitioners who provide care to their residents. What will enforcement of abortion criminalization look like in the age of tank-driving county cops with military-grade weaponry and budgets flush with “extra” COVID funding? It is not uncommon for clinics, especially in populous liberal cities, to establish friendly relationships with local law enforcement for “protection” from anti-abortion harassment and clinic protests. However, the abortion rights movement must concern itself with the realities of violent law enforcement and routine police suppression of activist struggles for justice, as we enter into this next horrific chapter of our decades-long fight. The police have not, do not, and will not protect us.
The Criminalization of Trans Existence
Parallel to abortion bans, the Right has been trying a variety of methods to criminalize trans existence through legislation. Restricting access to bathrooms and participation in youth sports has been common across the country. Approximately twenty-one states have introduced legislation in the last five years policing what restroom an individual can use on the basis of their gender presentation and the plaque on the door. Newly introduced legislation to ban trans kids from playing on gendered sports teams is pending in a number of states currently, while fifteen states already have those laws in place at the time of this writing.
Trans sports bans are rooted in and intertwined with athletics’ history of targeting Black women for being “too masculine,” performing “sex testing” and now capping the amount of endogenous testosterone in a female athlete’s body in order to compete.1Two-time Olympic gold medal winner Caster Semenya is a Black female athlete whose body produces more testosterone than “typically” seen in other cis women’s bodies due to a difference of sexual development. Semenya and other athletes like her are required, per World Athletics 2019 rules, to take testosterone-blocking medications to compete in many events. At the time of the rule change, Semenya was one of three African female athletes impacted by the change. She lost two appeals and is now bringing her discrimination case to the European Court of Human Rights.
Both the criminalization of abortion and the criminalization of trans existence disproportionately have negative, life-threatening, and fatal impacts on women of color.
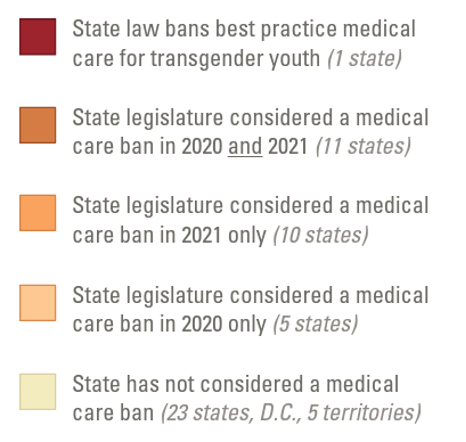
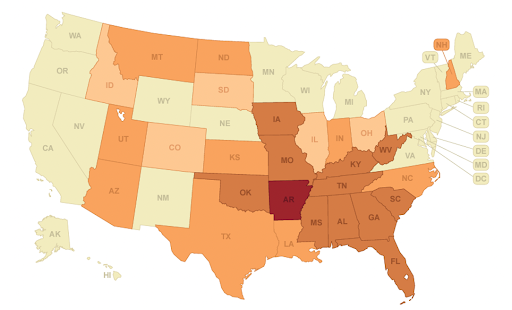
The Right’s current crusade against healthcare for trans young people clearly shows how abortion rights and trans liberation are inextricably linked. In 2021, twenty-two states introduced legislation prohibiting access to care for trans youth, thirteen of which also included criminal penalties for prescribing providers. Only Arkansas passed such legislation–the Save Adolescents from Experimentation (SAFE) Act–the first law in the country banning gender-affirming care for trans youth. A judge temporarily delayed the enactment of the bill thanks to a lawsuit from the ACLU, but the final verdict has yet to be decided.
On May 8, 2022, the Vulnerable Child Compassion and Protection Act was passed in Alabama, making the prescription of gender-affirming hormone therapy to minors a Class C felony—the first law in the country to criminalize gender-affirming care provision for youth. Once again, a temporary injunction was issued by an Alabama judge, citing the lack of evidence presented by the legislation and the abundance of evidence from numerous professional organizations on the benefits of said care. Alabama’s law sets new precedent above and beyond its transphobic intentions—healthcare provision has never been explicitly criminalized in this way, with the new assault on abortion care being the notable exception.
Missouri lawmakers have introduced a SAFE Act of their own, and, while debating it in April 2022, suggested that the ban be extended from those under 18 to those under 25, citing the continued brain development which occurs up to that age. It should not come as a surprise that healthcare bans imposed on youth herald a near-future in which adult care is also restricted, banned or criminalized. We should not be surprised; we should be enraged and terrified.
While some politicians in other states have publicly condemned these bans, no state has gone so far as to explicitly codify a right to gender-affirming care for all persons, including youth.
Several bills specific to youth are being considered in other states for the 2022 session. Idaho House Bill 675 used the term “genital mutilation” to mischaracterize gender-affirming care (GAC), and attempted to criminalize leaving the state to obtain gender-affirming care for a young person. HB675 passed the house but died in the Senate on the grounds of “undermining parental rights,” though the Republican Caucus made sure to make their strong condemnation of GAC known. “Parental rights” being inviolable by the state is a curious argument from the party seeking to end bodily autonomy for pregnant people whom the party already considers to be parents since conception.
Texas governor Greg Abbott’s February 2022 executive order quite prominently moved to criminalize parents supporting and facilitating their children’s healthcare. On May 13, 2022, the Texas Supreme Court upheld that gender-affirming healthcare for trans youth is worthy of child abuse investigations. This has expanded the possible state punishment from patients and providers—the abortion template—to now include parents. Again, this strategy is clearly patterned after SB8 where civilians are unofficially deputized to suspect and report parents of trans kids who may be guilty of providing loving support and gender affirmation.
While some politicians in other states have publicly condemned these bans, no state has gone so far as to explicitly codify a right to gender-affirming care for all persons, including youth. In this way, the trans liberation movement has more ground to gain, and can pattern our demands after gains made by the abortion rights movement. The Right is not the only movement where strategies can be shared.
Gender
Gender was differentiated from sex as a concept by feminists scholars in the 1970s. Gender refers to characteristics usually presumed to be associated with masculinity or femininity, which an individual has within them and expresses through their personality and behaviors. Gender is both socially constructed and a fundamental way that people understand themselves, move through the world, and structure their relationships.
Core to the Western colonial definition of “gender” is the gender binary, the concept that there are only two genders—man and woman—and only two gender expressions—masculine and feminine. Within the gender binary, people may feel themselves to have some combination of masculine and feminine, might be more or less one or the other, or strictly male or female. But the binary limits the total number of possible gender/identities to two. In truth of course, gender identities are beautifully infinite, as defined by visionary poet ALOK.
The art project “GENDER IS OVER (if you want it)” was inspired by John Lennon and Yoko Ono’s iconic billboard “WAR IS OVER (if you want it).” It places a fine point on the social construction and inherent harms of gender norms. However, it is important to complicate that assertion by specifying that binary gender is over (if we want it). Gender as a self-concept and complex relationship to body, self, and others is truly infinite. To achieve liberation, we don’t necessarily need gender to be over—we need the way that gender oppression functions in society to be over. We need the gender binary to be over.
Gender-Based Oppression
Why is there gender-based oppression? And why do conservatives crave it so? Gender is a method of categorization and social control. Pre-colonization, many Indigenous cultures and societies understood and defined gender quite differently than Western colonizers. Gender is not and was not binary for many Indigenous peoples. Western colonization has enforced binary gender because it serves the imperial, white supremacist project, similar in utility to the social definitions of race and class. These supposed divisions and “opposing” identities divide society to help the ruling class maintain power. Under capitalism, gender roles reinforce a labor divide to preserve an unpaid domestic work force.
Gender roles are very valuable to class society. Valuable here literally meaning value and profit are better extracted when a gender binary organizes work in and outside of the home. Social reproduction theory asserts that while waged labor outside the home is what produces profit and wealth for the ruling class, its existence is dependent on unwaged labor inside the home. Unpaid domestic labor has historically been feminized. All the things upon which the maintenance and reproduction of waged labor depend—cooking, cleaning, clothing, and “producing” (i.e. growing and birthing) actual human babies—fell to femmes. Without unwaged domestic work, wage labor is nearly impossible, as food, sleep, housing, and clothing are all required to continue to live and function in a waged work environment. US capitalism relies heavily on trillions’ of dollars of unpaid work to keep workers showing up to jobs for pay.
Keeping women and feminine individuals in unpaid domestic work has been accomplished through the maintenance of binary gender roles within the nuclear family.
The profits of the ruling class depend on half the planet not expecting or demanding wages for social reproductive labor. Keeping women and feminine individuals in unpaid domestic work has been accomplished through the maintenance of binary gender roles within the nuclear family. The structure of the nuclear family and its dumping of domestic labor responsibilities on the back of one or more feminine individuals within the home is a highly effective way for those in power to increase their wealth, as well as to keep the working class exhausted and less capable of participating in uprisings and their overthrow. Femmes are compelled to continue in this way for a variety of reasons—care and love for their families, social expectation, deeply internalized misogynist/homophobic/transphobic rhetoric, abuse, and explicit violence. Those who depend on binary gender roles have attempted to find biological, historical, evolutionary, and moral justifications for them. Yet they have everything to do with power, patriarchy and capitalism, and those sure as hell can be over (if we want it).
“Reproduction” as a medicalized human function meaning “sex and babies” has a whole new ring to it when you apply the clarifying lens of Marxist theory. Social reproduction theory shows unequivocally that reproductive justice could not be more intimately linked to the need for a revolutionary labor movement.
Family Values
The Right launches similar attacks on abortion rights and queer and trans existence using the concept of “family values.” The nuclear family is also a construction of colonized Western society. Forced monogamy and individualized units of blood relatives ensured that property was inherited patrilineally, thus protecting generational wealth and the supremacy of the genocidal white men in power. Perhaps this is why many queer, trans, and pro-abortion feminists are more than happy to be accused of degrading “traditional family values” and “destroying America” as these ideas (and the country which peddles them) are repellent and oppressive.
Frederick Engels wrote in The Origin of the Family, Private Property and the State: “The origin of monogamy […] was not in any way the fruit of individual sex-love, with which it had nothing whatever to do; marriages remained as before marriages of convenience. It was the first form of the family to be based, not on natural, but on economic conditions – on the victory of private property over primitive, natural communal property.” And what’s a family without babies (heirs), babies (workers) and more babies (ballasts anchoring birthing people to the home)!
Abortion threatens the status quo not only because it upends “family values” and gets the Religious Right in a tizzy. If people who can get pregnant are in charge of their reproductive futures, then they can refuse participation in forced birth and unpaid labor which largely functions in the service of cisgender men and their bosses (usually more cis men). Trans existence similarly threatens the status quo because not conforming to binary gender complicates this supposedly “natural” labor divide. Challenging these dominant norms may lead first to questioning the supremacy of the patriarchal, white ruling class, and then destroying it by uniting the multigender, multiracial working class to take our rightful power.
Historical Background: Abortion
There has been abortion for as long as there has been birth. It is a common misconception that the Christian and Catholic churches have always stood in moral opposition to abortion. White male clergy decreed that abortion was a-okay until a fetus had a soul, and they decided that “ensoulment” happened at 166 days, which is approximately twenty-three weeks of pregnancy. Interestingly, now with the technology to confirm, we know that to actually be the approximate date of viability. (So good work, old white dudes who could read.) Before the nineteenth century, support for pre-viability abortions was the Catholic church’s position for 278 years.
Abortion was also no big deal in the early United States. According to the Guttmacher Institute, in-clinic abortion “was made illegal under most circumstances in most states beginning in the mid-1800s.” This coincided with the sea change in the Catholic church. In the 1960s, the women’s liberation movement began mobilizing around abortion rights. In response, individual states began reforming anti-abortion laws, resulting in seventeen states permitting abortion in some circumstances prior to Roe v. Wade.
There has been abortion for as long as there has been birth.
The Religious Right was not morally outraged by abortion until a concerted, years-long campaign started in 1979, six years after Roe was handed down. The campaign was engineered by conservative New Right activist Paul Weyrich who believed tapping the evangelical voting bloc could build power for conservative politics. Evangelicals were riled by religious schools losing tax-exempt status for refusing racial integration. Weyrich viewed their inflammation as the launch point he’d been waiting for. He wanted to stop President Carter’s re-election and better protect white supremacists against the so-called “liberal agenda” and sneaky communists. They ultimately failed to legally enshrine racially segregated schools. However, while the movement Weyrich led was slow to embrace anti-abortion ideology, they quickly embraced anti-abortion extremism, ushering in the anti-abortion domestic terrorism which marred the movement for much of the 1980s and 90s, with lasting fascist reverberations.
What Is Abortion?
Abortion is commonly used in political rhetoric as a moral talking point and rallying cry, but it is just an ordinary and common procedure that nearly one in every four people who can get pregnant have by the age of forty-five.
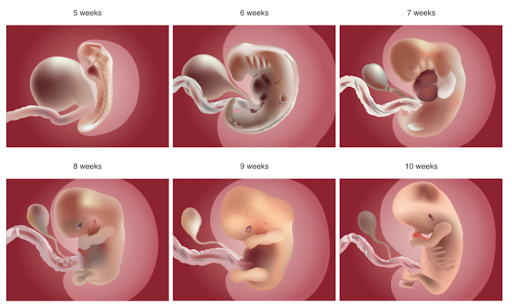
So what is abortion? The Right has used imagery to great effect of supposed “post-abortion” bloody fetuses blown up on posters and billboards. They also delight in promoting their messages alongside pictures of actual living children, smiling and sparkling in their baby-ness, with medically inaccurate sayings like “I could smile 12 weeks after conception” or “Dad’s princess #<3beat at 18 days.” Eight-six percent of abortions in the United States happen in the first trimester of pregnancy, fifty percent before eight weeks and thirty-six percent between eight and twelve weeks. At this stage of development, human embryos are visually indistinguishable from those of a donkey or an elephant.
Needless to say, smiling—a human emotional reaction—is something these cell clusters are incapable of; and, as all immature embryonic organs are little more than microscopic tubes, they have no hearts, much less heartbeats. But scientifically accurate imagery of involuntary, primitive “facial” twitches and electric pulses in a tiny tube would do markedly less to manipulate pregnant people and galvanize outrage against abortion.
While it is important to accurately represent what the average abortion truly is, we must also be unequivocal in our support of abortions at all stages of pregnancy, even when an embryo or fetus is more recognizable as of our species. Early abortion is preferrable to many as it has fewer complications, is less painful, and is less expensive than later abortion. Access to later abortion must be vigilantly defended and protected, as it is no less necessary or life-saving for pregnant people. Abortion restrictions are often major contributors as to why individuals have abortions later in pregnancy—mandatory twenty-four-hour waiting periods, mandatory ultrasounds, far-distant clinics, and the required money, time off work, childcare, and 2–3 hours for an in-person appointment.
COVID emergency exemptions enabled the prescription and shipment of abortion medications in many states without in-person care. On December 15, 2021, after many years of activist work, the FDA lifted a previous restriction on mail-order abortion medications, securing the continuation of new abortion telehealth companies and the adoption of telehealth by well-established providers across the country. While there are still unnecessary restrictions even with this landmark decision (only specially certified pharmacies can send abortion medications), with telehealth abortion access, more and more people are able to have abortions as early as possible in their pregnancies. It’s considerably easier and more feasible for most to have an abortion when there is immediate access to care—no wait for an appointment, no required ultrasound or mandatory waiting period, no work absence or childcare arrangements. Plus it is more discrete if you are trying to maintain privacy from a partner or family member—or that lady at church who wants to get you arrested for murder.
How can anti-abortion activists claim to protect life when their desired criminalizations will result in the mass death of currently alive, fully formed people?
Abortions have changed medically in the almost five decades since Roe. Modern abortion is much safer than carrying a pregnancy to term and childbirth. A pregnant person is fourteen times more likely to die in childbirth than to die from complications of a safe abortion, according to a 2012 study which reviewed US mortality rates associated with both from 1998–2005. One study showed that there would be an estimated twenty-one percent increase in pregnancy-related deaths by the second year of a nationwide abortion ban. The numbers increase to thirty-three percent for Black women specifically, which parallels racist health inequities and existing disproportionate mortality rates for birthing Black people. Notably, these numbers parallel another older set of statistics: before Roe was the law of the land, illegal abortion was twelve times more likely to kill women of color.
Not only can the United States expect increased pregnancy-related deaths in a post-Roe future, but there will still be many people without access to accurate medical information, or awareness of safe self-managed abortion strategies and care providers, like Plan C and Aid Access. While in 2022 coat hanger imagery no longer represents the majority of self-managed abortion in the United States, there will still be many individuals for whom self-induced abortion will result in debilitating or fatal medical emergencies.
How can anti-abortion activists claim to protect life when their desired criminalizations will result in the mass death of currently alive, fully formed people?
Historical Background: Transgender Care
Gender diversity and the infinity of gender identities have also existed since humans were born. The recorded history of gender-affirming healthcare does not necessarily begin with the work of Dr. Magnus Hirschfeld, but he is a prominent signpost. Dr. Hirschfeld founded the Institut für Sexualwissenschaft (Institute for the Science of Sexuality) in Berlin which studied queerness and trans identity in a radically positive way. Opened in 1919, the Institute was unapologetically pro-queer and pro-trans. It offered education, conducted research, and provided medical services to a broad community. It also housed many prominent leftists and well-known transgender individuals of the time. In 1933, a Nazi student organization looted the Institute and burned all the books and research it contained. Despite this, Hirschfeld’s work was seminal to the establishment of Western protocols for medical gender transitions.
The first formal protocols for gender-affirming hormone therapy were published in 1979 by the Harry Benjamin International Gender Dysphoria Association, now known as the World Professional Association of Transgender Health (WPATH). Dr. Benjamin was a German-American endocrinologist who, early in his career, studied sexology with Dr. Hirschfeld in Germany. After moving to the United States, Benjamin ended up in radical sex-positive circles (for that era) with Margaret Sanger, founder of Planned Parenthood, and Dr. Alfred Kinsey, famed progessive sexologist. Hormone provision and gender-affirming medicine was happening well before 1979, and likely predated Hirschfeld’s Institute, but WPATH’s Standards of Care were the first published professional guidelines for health care providers.
In 1979, the Harry Benjamin Protocols were considered radical and boundary-pushing, but became outdated in the following decades. Unfortunately those protocols stayed prominent until WPATH’s 7th version of Standards of Care, published in 2012, which included support for an informed consent model of care. There are now additional expert guidelines to reference from other professional organizations, including the University of California at San Francisco Center of Excellence for Transgender Health and the Endocrine Society. All of these guidelines have blindspots and need updating with more direct input and authorship from the trans and nonbinary communities. But there is indisputable professional consensus that gender-affirming care is strongly supported by scientific research, and profoundly beneficial for transgender and nonbinary people.
There are approximately one million trans adults in the United States, though it’s likely this is an underestimation. More recent research shows that two percent of US high school students identify as trans or nonbinary. There is a highly disproportionate rate of suicidality, self harm, and attempted suicide among trans and nonbinary youth. Several research studies have supported that access to gender-affirming care, including hormone therapy initiated during adolescence, has been associated with lower incidence of suicidal ideation and attempted suicide.
If the Right really wants a lot of babies to stay alive, supporting trans youth’s access to life-saving care would be an excellent place to start.
What Is Gender-Affirming Care?
So what is gender-affirming care for trans youth? Conservatives assert that gender-affirming care is a form of child abuse, which involves experimentation, involuntary surgeries, and the infliction of forcible permanent changes to young people’s bodies. Gender-affirming care for all ages typically begins with a variety of non-permanent, reversible, or changeable voluntary decisions, namely social transition—how you present yourself to the world with clothes, your name, pronouns, hairstyles, makeup, etc., and legal transition—changing your name legally, changing your gender marker legally, updating your legal documents. This can be done as early in childhood as you would like, and a child might change those things multiple times, change them back to what they used to be, or keep them forever. There is potential for fluidity and self-exploration without permanence or harm.
The earliest medical intervention for trans youth is pubertal suppression, which is possible prior to the onset of puberty (usually between eight and twelve years old) through age seventeen. Pubertal suppression means using medications that temporarily delay puberty to buy young people time to sort through how they’d like to develop physically, whether they want certain secondary sex characteristics, which ones they want, and when. The introduction of hormone therapy is not typically initiated until a person is at least age sixteen, though in some cases this may happen a year or two earlier with extensive parental involvement. Anyone under age eighteen will only be able to access pubertal suppression or gender-affirming medications with parental consent from all legal guardians, typically both biological parents regardless of their marital or relationship status. Gender-affirming surgeries generally don’t happen until someone is eighteen and can consent to those treatments independently.2 The legal injunction against Alabama’s law still supports the ban on gender-affirming surgeries for minors, even though care providers there maintain that such surgeries for minors are not performed in the state of Alabama.
Accessing gender-affirming care as a young person is already incredibly difficult, beyond parental consent and medical clearance. There are few providers who manage medical transition for anyone, let alone minors, especially in the Southeast and Midwest. Gender-affirming care, medications, and surgeries are prohibitively expensive even for most adults, and rarely covered by private or public insurance (though coverage has improved in some states and through some insurance carriers). Some of the attempted bans seek to make coverage of care through insurance illegal as well. Right-wing lawmakers yelling about genital mutilation and child endangerment have literally no idea what gender-affirming care is.
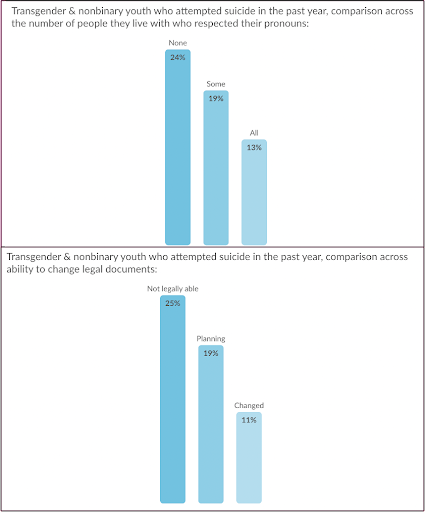
It doesn’t even take hormones or pubertal suppression to positively impact the mental and emotional health of trans young people. A 2021 survey from The Trevor Project showed trans and nonbinary youth who reported having their pronouns respected by all the people they lived with attempted suicide at half the rate of those who did not. The ability to change their name or gender marker on legal documents and access to gender-affirming spaces also lowered rates of suicide attempts. While gender-affirming medical interventions like pubertal suppression and hormone therapy improve trans patient outcomes remarkably, non-permanent, non-invasive, non-medical behavioral and social practices have just as much impact on the quality of life and health of trans young people.
If the Right truly cared about the health and well-being of transgender youth, they would vociferously champion access to gender-affirming care, as the alternatives are deadly.
Trying to win the race to the bottom, in April 2022, Florida’s surgeon general, Joseph Ladapo, issued new guidelines from the Florida Department of Health against not only medical transition for youth but social transition as well. The guidelines state, “social gender transition should not be a treatment option for children or adolescents,” and suggest alternative “treatment” options of “counseling” and “social support.” As the state attempts to restrict all care providers from affirming trans identities for young people, one can assume that the only remaining “counseling” alternative would be a form of conversion therapy. A 2018 study showed that LGBT individuals who had been subjected to conversion therapies had double the risk of attempted suicide compared to LGBT individuals who had not.
If the Right truly cared about the health and well-being of transgender youth, they would vociferously champion access to gender-affirming care, as the alternatives are deadly.
Shared Strategies
How does the Right use these same strategies to attack both abortion and trans healthcare? One shared overall strategy is punting the responsibility and legality of these rights from federal court to individual states. Allowing states to regulate this life-saving care instead of blanket federal protections creates more opportunities to challenge, restrict, and ban access. Another strategy they love is introducing extremist bills that they expect not to pass but with the intention of advancing their agenda and inflaming public discourse. They also share templates to introduce copycat bills in every possible state where the political climate might be favorable. In the case of abortion, many of these bills have been introduced in the hope of a legal fight that advances to the Supreme Court to pose a direct challenge to Roe. This is where we now find ourselves with Dobbs vs Jackson.
Missouri House Bill 2810 is a salient example of extremist tactics. The criminalization of ectopic pregnancy treatment was never the goal. Including it in the bill made felony charges for providers seem reasonable by comparison. Their willingness to remove extremist propositions helps them look cooperative and willing to compromise across the aisle. Even when their bills are not passed or they lose court cases, often the Right will reframe the same arguments in new bills and get them back into the courts, retreading the same ground over and over again, hoping to finally win.
The shared basis of gender oppression enabling the use of shared attack strategies means the language in abortion bans can easily be transformed into language used in trans healthcare bans.
Extreme attacks on the most fundamental aspects of public life—using a restroom or a water fountain—have also been Right-wing strategies to create a hostile and dangerous environment for the targeted communities. Many on social media saw connections with the Jim Crow laws of the South during the first wave of Bathroom Bills, saying that it’s never been about bathrooms, just like it was never about water fountains. It is about using racist and transphobic fearmongering to restrict non-white, non-cisgender, non-heterosexual participation in society, and further building conservative power.
The shared basis of gender oppression enabling the use of shared attack strategies means the language in abortion bans can easily be transformed into language used in trans healthcare bans. As always, Texas is a prime example. Senate Bill 8 emboldens civilians to become law enforcement, and turn in their neighbors or providers to be criminally prosecuted for abortion care. Governor Abbott’s executive order on trans youth, upheld by the state supreme court is essentially the same: rat out your neighbors for trying to take care of their kids and the state will arrest them.
Impact of Bans on Providers
These waves of criminalization for both abortion and gender-affirming care primarily target providers for state punishment, not patients. This has long been a part of the Right’s policy playbook and political strategy. Criminalization of care provision can be more easily evidenced than proving one received it, making it easier to bring charges against a provider than a patient (though there are many horrifying examples of states detaining people, usually at the point of care, who were suspected of having abortions). Attempts to criminalize providers also discourage new providers, students, and existing providers from training and providing both forms of care for fear of state and community retribution. Thus there is a critical shortage of care providers for both types of care, and fewer and fewer providers are learning to do it.
The assassination of Dr. George Tiller in 2009 left only four physicians in the United States trained to provide third trimester abortions. The providers of third trimester abortions offer the most compassionate and supportive care to their patients and patients’ families, worlds apart from the medically inaccurate and vulgar language used by the Right to frame later abortion. These procedures are akin to fetal hospice, facilitating the end of a pregnancy as gently and thoughtfully as possible. For more on the complexity and care of third trimester abortion, watch the 2013 documentary, “After Tiller,” which intimately follows and interviews the remaining providers after Tiller’s assassination.3For more on the complexity and care of third trimester abortion, watch the 2013 documentary, “After Tiller,” which intimately follows and interviews the remaining providers after Tiller’s assassination.
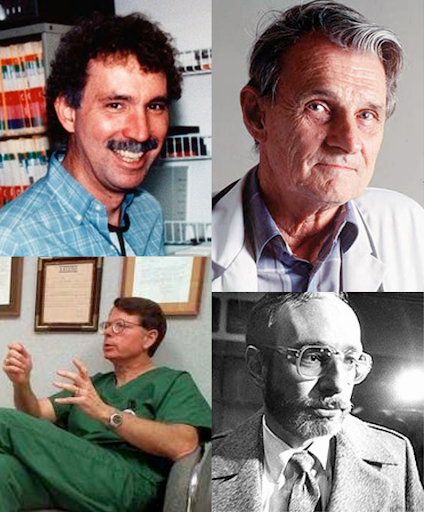
Since 1977 in the United States and Canada, anti-abortion terrorists have murdered eleven people and attempted to murder seventeen. They are responsible for 383 death threats, 153 physical assaults, 373 clinic invasions, 41 bombings, 655 anthrax threats, and 3 kidnappings. National Abortion Provider Appreciation Day commemorates the assassination of Dr. David Gunn, the first abortion provider to be assassinated in the US on March 10, 1993. Routine harassment of clinic staff and providers by anti-abortion protestors is considered an expected hazard of the job. Providers specifically are doxxed, followed and even their families and children are terrorized.
In addition to explicit violence toward providers, the anti-abortion movement opens fake clinics which confuse and endanger patients while interfering with safe care provision at real ones. Crisis pregnancy centers (CPCs) lure pregnant people in with free pregnancy tests and free ultrasounds, but their purpose is to coerce and shame people into staying pregnant. They are not medical facilities and do not provide any medical services. In some states, legislation has been passed mandating that CPCs post visible notices stating that they do not provide medical care or abortions and that they do not have medical care providers. CPCs are the recipients of federal and state funds that would otherwise go to sex education and actual reproductive health services. As a particularly insidious tactic, anti-abortion organizations attempt to build or open CPCs as close to real abortion providers as possible to trick patients into entering them for appointments nearby.
A queer corollary to CPCs would be conversion therapy, the abusive programs targeting LGBTQ youth to shame and traumatize them based on their sexuality or gender presentation. Unfortunately, the field of medicine also has a history of destructive medical and surgical interventions to try to “cure” homosexuality and gender diversity. The most horrendous example of abusive medical intervention may be the practice of genital surgeries starting at birth to permanently alter intersex children’s bodies well before informing or consenting them is possible. The fear-mongering false claims from the Right about gender-affirming care for young people—genital mutilation, permanent physical changes, abusive medical practice—actually happen to babies and young people with intersex traits in an attempt to uphold the biological defense for binary gender. It is heinous and there is a vibrant movement to end it. How grumpy the Right must be that not only are there more than two genders, there are more than two sexes!
There are fewer direct comparisons between attacks on abortion providers and attacks on queer and trans care providers. The latter have experienced profound discrimination and harassment due to the identities of their patients and the perceived risk of care provision, especially regarding HIV/AIDS. Much more common though are acts of violence aimed at queer and trans people themselves, sometimes in the context of care environments. There is an epidemic of fatal violence against transgender women of color with more casualties every year. 2021 was the deadliest year on record for trans people in the United States. Transgender people are over four times more likely to experience violence than cisgender people, including rape and sexual assault.
Criminalization of healthcare provision, whatever that care might be, results in overwhelmed, targeted and unsafe providers as well as patients. If this country continues to criminalize gender-affirming hormone therapy and care, the impact on trans care providers will be profound. If trans care continues to follow the political trajectory of abortion, there will be even higher risks for similar types of harassment, discrimination, and violence.
Right Now
The reality of the political landscape right now is that the Right is trying to kill people—people who can get pregnant, Black and brown people, Indigenous people, transgender and nonbinary people—and it is up to us to fight back. Feeling overwhelmed and defeated is understandable as the Right is indisputably winning, even as fierce, new youth-led movements revive and revise our losing side in powerful necessary ways. If anyone can turn this boat around, it will be the formidable, brilliant, radical young people who have grown up in the midst of escalating climate catastrophe, endless wars, commonplace mass shootings, and a deadly global pandemic. We also have historical examples from our movement ancestors who fought worse things and won.
Roe was not the result of an objective interpretation of the US constitution on the part of the 1973 Supreme Court. Roe was a product of sustained and arduous struggle. We won that decision under President Nixon, an anti-abortion Republican, with a conservative majority in the Supreme Court. We won because there was a militant, multiracial feminist movement in the streets, forcing the public to address the realities of criminalization and forcing the hand of politicians and pundits to acknowledge majority support for abortion rights.
Currently both the abortion rights movement and the queer and trans liberation movements have been commandeered by nonprofits and prominent national service providers. These corporate institutions dominate the public discourse with weak liberal axioms as they kowtow to and shill for the Democratic Party, funneling rage and momentum to the polls. The Supreme Court leak more than adequately illustrates that the cowards at the reins of our movements have chained themselves to a losing strategy. The nonprofit and national care organizations raking in donations as Roe is poised to fall have never met a fight they couldn’t limply lose. Gay Inc. has put very little of their money or energy into protecting trans kids but are starting to fret about their precious marriage equality as the Supreme Court shows its fangs.
We won Roe under President Nixon, an anti-abortion Republican with a conservative majority in the Supreme Court, because of a militant, multi-racial feminist movement in the streets.
We must take back leadership of our own movements, movements we started with brave rebellions and collective care, movements which will only win if our communities are controlling them from below. Mass organizing reproductive and trans healthcare workers into labor unions could shift movement strategy and leadership directly into our own hands. Not only would unions better protect workers’ safety from violence and legal attacks, collective organization and worker power could bring the backbone and teeth to our movements currently lacking in light of their corporate leadership.
Critical to our survival in these treacherous times are organizations which offer material support—organizations which assist abortion travellers with housing, transportation, and emotional support; abortion funds; community groups and care providers protecting and welcoming trans youth and their families. Yet the political moment also demands incisive and visionary political strategy to forge ahead. In this we are fortunate to have robust, inspiring historical examples.
The Combahee River Collective was founded by a group of radical Black feminists in 1974. They were, in their own words, “actively committed to struggling against racial, sexual, heterosexual, and class oppression, and see as our particular task the development of integrated analysis and practice based upon the fact that the major systems of oppression are interlocking.” SisterSong is an organization which moves in that same tradition and developed the Reproductive Justice framework in 1994 on which the abortion movement depends. From Chicago, there is the vital legacy of the Jane Underground Abortion Collective, a group of volunteers who provided over 11,000 safe but illegal abortions pre-Roe. Multiple online care organizations have taken up their mantle—Plan C, Aid Access, Women on Web—providing mail-order abortion medications in states or countries where abortion is illegal or heavily restricted.
Ancestors of queer and trans liberation are numerous and brilliant. ACT-UP, the AIDS Coalition to Unleash Power, is a direct action organization dedicated to increasing access to HIV and AIDS care, especially for queer and trans people. There is none more lovely than the STAR Collective, Street Transvestite Action Revolutionaries, founded by our beautiful foremothers Marsha P. Johnson and Sylvia Rivera, best known for starting the Stonewall rebellion. Carrying on that radical tradition is the Brave Space Alliance in Chicago, which provides material support and advocacy for Black, Indigenous, and people of color who identify as trans. Out of Atlanta, Southerners On New Ground describes itself as “a home for LGBTQ liberation across all lines of race, class, abilities, age, culture, gender, and sexuality in the South.”
Additionally, there are historical examples of how queer and trans liberation activists have shown up in solidarity with other movements which they’ve recognized as intrinsically linked to their freedom. Church Ladies for Choice, founded by ACT-UP members in 1991, was a drag troupe that came out fighting with the feminist movement for abortion rights. Lesbians and Gays Support the Miners was a UK-based group started by young communist queers who fought to support striking miners under violent state repression from Margaret Thatcher.
This list is far from exhaustive, as many of the organizers to which we owe our gratitude and current freedoms were unsung, silenced, misgendered, incarcerated, and killed by violence and viruses. Our revolutionary ancestors were ordinary people with jobs and exes and illnesses, just like us. May their stories ring out in the streets as we educate one another and learn by their examples.
What’s Next
The next phase of this movement must rapidly evolve if we want to win. We must embrace intersectional, trans-inclusive feminism as the only way forward. We must build solidarity with the movement for Black lives, the labor movement, the anti-war movement, the immigrant rights movement, the climate justice movement, the disability justice movement, and the Indigenous liberation movement. Our next steps require diverse and synthesized tactics, just as the Right is coordinated and strategic in their many attacks. We need masses in the streets, masses providing mutual aid, masses grassroots organizing, voting, and facilitating access to care. None of these things on their own leads to collective liberation. It has to be everything and new things which have no historical precedent.
Our power is limitless when we fight together. I believe that we will win.
The goal of the abortion rights and trans liberation movements must be abolition, nothing less. There is no autonomy or safety for us under capitalism, colonialism, white supremacy, gender oppression, and ableism. So we must demand abolition. Police abolition to end the violent presence of cops at our clinics, in our communities, and against our movements. Prison abolition to end incarceration not only of care providers, patients, and parents but of all humankind—migrant children caged at borders and survivors of domestic violence to those whose offenses require compassionate restorative justice not torture and isolation. Billionaire abolition. Military abolition. White supremacy abolition. Global warming abolition. Gendered-violence abolition. Poverty abolition, which is of course capitalism abolition.
Our power is limitless when we fight together. I believe that we will win.
